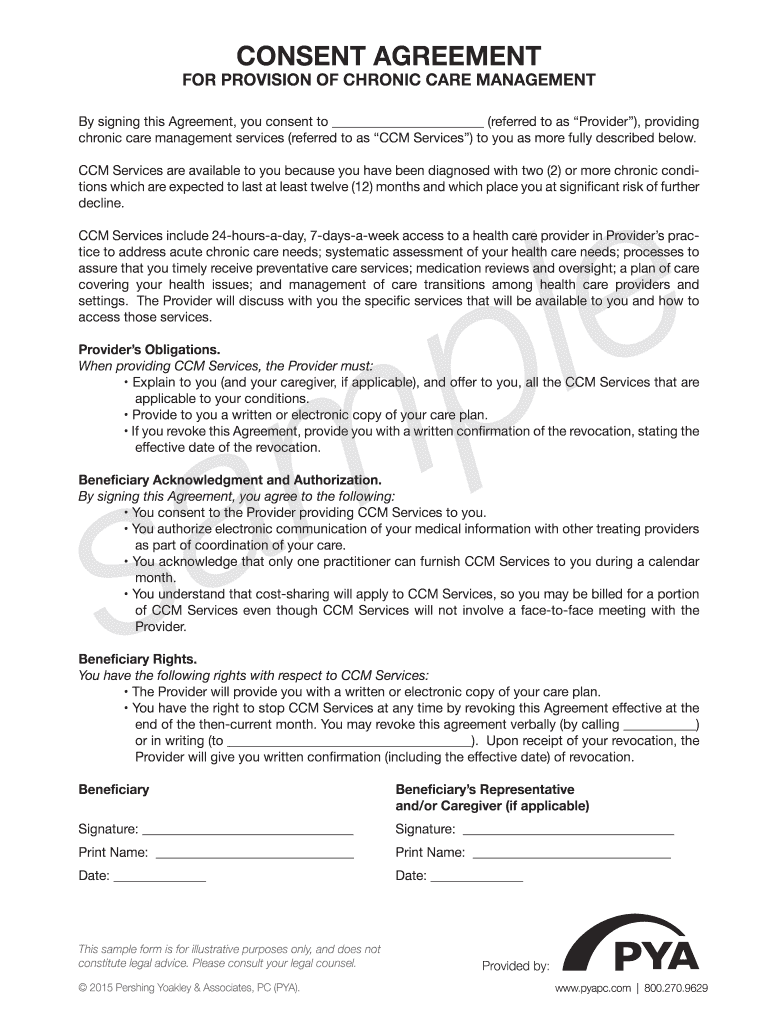
Ccm Consent Form - Because your signature is required to end your chronic care management services, please ask any of our staff members for the ccm termination. If another physician has offered to provide ccm, you will have to choose which physician is. You can only give ccm consent to one provider at a time. Ccm consent form i, ____________________________________, agree to the provision of chronic care management (ccm). By signing this agreement, i consent to receive these services and agree to the following: My provider has explained to me the availability and the elements. Your provider will then give you written confirmation, including the effective date of revocation.
Ccm consent form i, ____________________________________, agree to the provision of chronic care management (ccm). By signing this agreement, i consent to receive these services and agree to the following: If another physician has offered to provide ccm, you will have to choose which physician is. My provider has explained to me the availability and the elements. You can only give ccm consent to one provider at a time. Your provider will then give you written confirmation, including the effective date of revocation. Because your signature is required to end your chronic care management services, please ask any of our staff members for the ccm termination.
By signing this agreement, i consent to receive these services and agree to the following: Because your signature is required to end your chronic care management services, please ask any of our staff members for the ccm termination. You can only give ccm consent to one provider at a time. If another physician has offered to provide ccm, you will have to choose which physician is. Ccm consent form i, ____________________________________, agree to the provision of chronic care management (ccm). Your provider will then give you written confirmation, including the effective date of revocation. My provider has explained to me the availability and the elements.

CCMC Form PDF
By signing this agreement, i consent to receive these services and agree to the following: Your provider will then give you written confirmation, including the effective date of revocation. If another physician has offered to provide ccm, you will have to choose which physician is. Because your signature is required to end your chronic care management services, please ask any.

How to Complete the CCM Forms Case Management Society of Australia
By signing this agreement, i consent to receive these services and agree to the following: Because your signature is required to end your chronic care management services, please ask any of our staff members for the ccm termination. Ccm consent form i, ____________________________________, agree to the provision of chronic care management (ccm). You can only give ccm consent to one.

Chronic Care Management Program Carson Medical Group
By signing this agreement, i consent to receive these services and agree to the following: Ccm consent form i, ____________________________________, agree to the provision of chronic care management (ccm). If another physician has offered to provide ccm, you will have to choose which physician is. Your provider will then give you written confirmation, including the effective date of revocation. You.
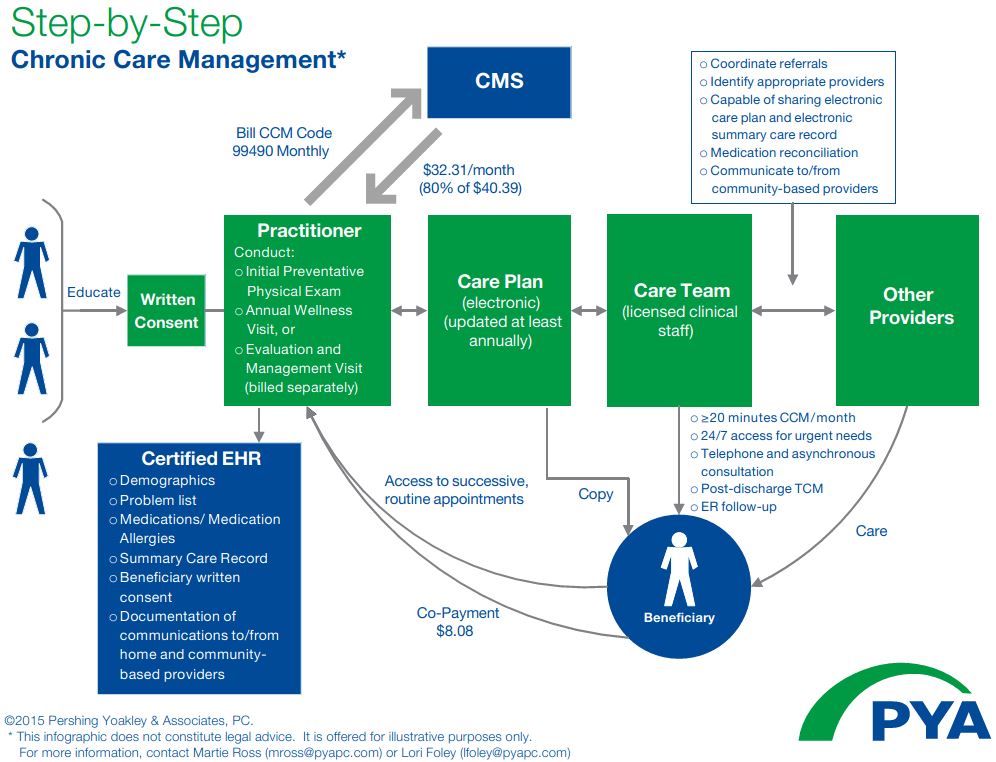
PYA Releases Chronic Care Management Infographic
My provider has explained to me the availability and the elements. Because your signature is required to end your chronic care management services, please ask any of our staff members for the ccm termination. You can only give ccm consent to one provider at a time. If another physician has offered to provide ccm, you will have to choose which.
Ccm Template
You can only give ccm consent to one provider at a time. Because your signature is required to end your chronic care management services, please ask any of our staff members for the ccm termination. By signing this agreement, i consent to receive these services and agree to the following: Ccm consent form i, ____________________________________, agree to the provision of.
Chronic Care Management Consent Form Fill Online, Printable, Fillable
You can only give ccm consent to one provider at a time. If another physician has offered to provide ccm, you will have to choose which physician is. Ccm consent form i, ____________________________________, agree to the provision of chronic care management (ccm). By signing this agreement, i consent to receive these services and agree to the following: Because your signature.

Chronic Care Management Program Carson Medical Group
If another physician has offered to provide ccm, you will have to choose which physician is. Because your signature is required to end your chronic care management services, please ask any of our staff members for the ccm termination. Ccm consent form i, ____________________________________, agree to the provision of chronic care management (ccm). By signing this agreement, i consent to.
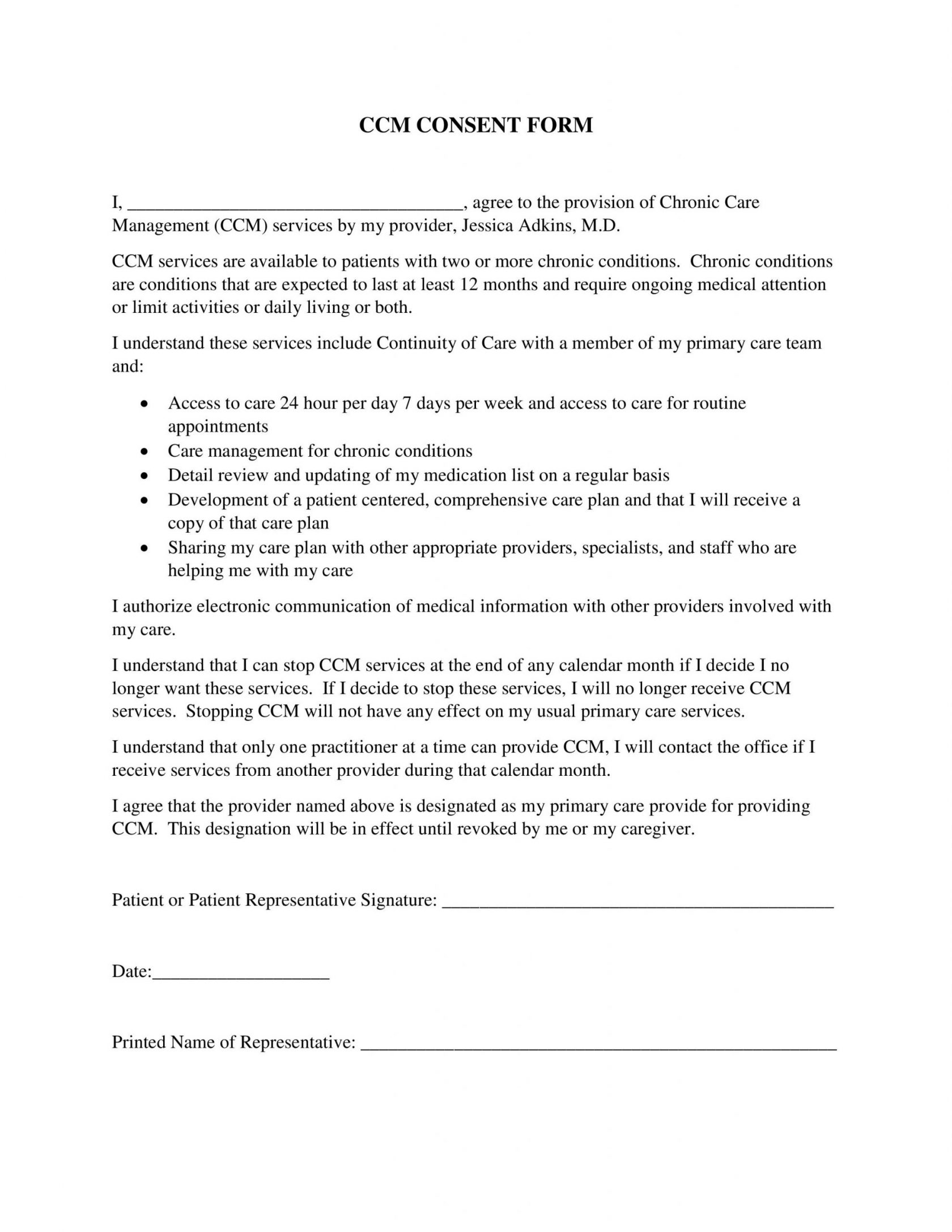
Forms Jessica Marie Adkins, MD Ventura County, CA Physician
You can only give ccm consent to one provider at a time. Ccm consent form i, ____________________________________, agree to the provision of chronic care management (ccm). Because your signature is required to end your chronic care management services, please ask any of our staff members for the ccm termination. My provider has explained to me the availability and the elements..
Statement of Compliance CCM Eligibility Requirements 1 Doc
By signing this agreement, i consent to receive these services and agree to the following: My provider has explained to me the availability and the elements. You can only give ccm consent to one provider at a time. If another physician has offered to provide ccm, you will have to choose which physician is. Because your signature is required to.
.png)
Chronic Care Management (CCM) Reference Card
Ccm consent form i, ____________________________________, agree to the provision of chronic care management (ccm). You can only give ccm consent to one provider at a time. By signing this agreement, i consent to receive these services and agree to the following: My provider has explained to me the availability and the elements. Because your signature is required to end your.
If Another Physician Has Offered To Provide Ccm, You Will Have To Choose Which Physician Is.
You can only give ccm consent to one provider at a time. Ccm consent form i, ____________________________________, agree to the provision of chronic care management (ccm). My provider has explained to me the availability and the elements. Your provider will then give you written confirmation, including the effective date of revocation.
By Signing This Agreement, I Consent To Receive These Services And Agree To The Following:
Because your signature is required to end your chronic care management services, please ask any of our staff members for the ccm termination.