Hipaa Form Pdf - Authorize this release to extend to all aspects of testing, diagnosis or treatment. Free immediate download of medical relasese form pdf. A hipaa authorization form must be obtained from a patient before their protected health. I expressly request that the designated record custodian of all covered entities under hipaa identified above disclose full and complete. Exclude the following information (initial): This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa).
This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa). A hipaa authorization form must be obtained from a patient before their protected health. Exclude the following information (initial): I expressly request that the designated record custodian of all covered entities under hipaa identified above disclose full and complete. Authorize this release to extend to all aspects of testing, diagnosis or treatment. Free immediate download of medical relasese form pdf.
Exclude the following information (initial): I expressly request that the designated record custodian of all covered entities under hipaa identified above disclose full and complete. Free immediate download of medical relasese form pdf. A hipaa authorization form must be obtained from a patient before their protected health. Authorize this release to extend to all aspects of testing, diagnosis or treatment. This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa).
HIPAA Medical Release Form & Example Free PDF Download
Exclude the following information (initial): This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa). I expressly request that the designated record custodian of all covered entities under hipaa identified above disclose full and complete. Authorize this release to extend to all aspects of testing, diagnosis or.
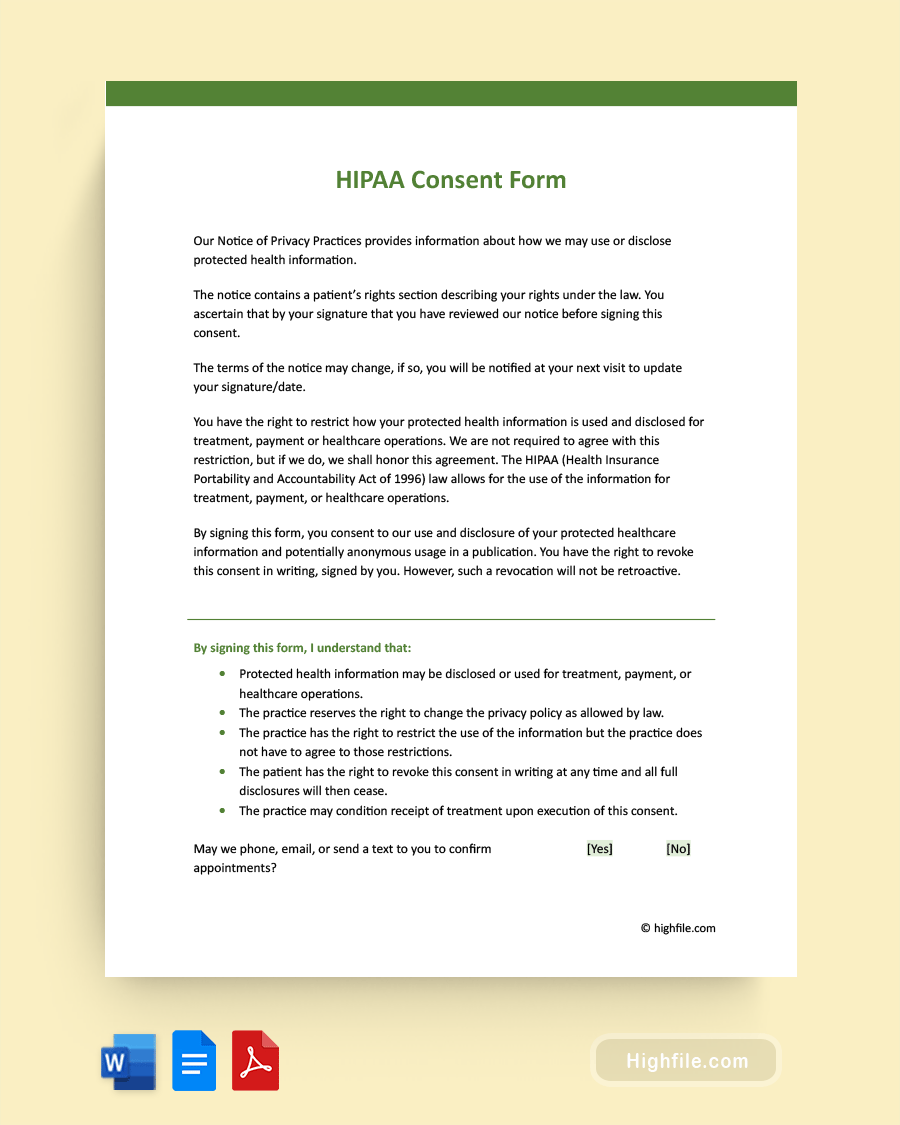
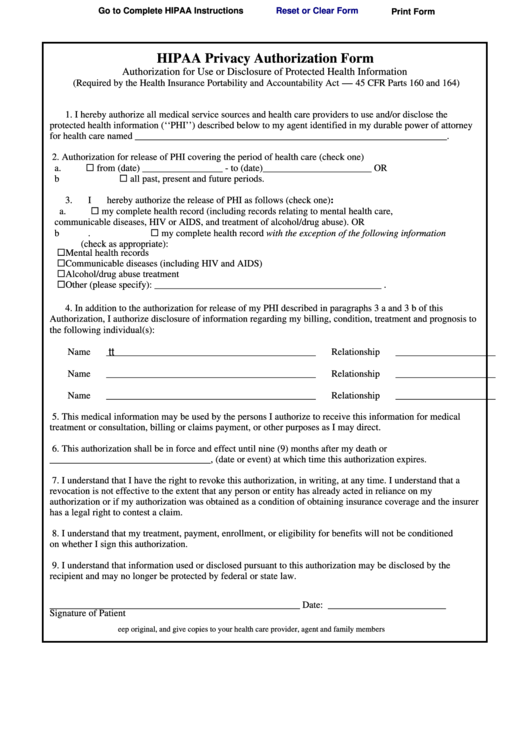
HIPAA Consent Form Word PDF Google Docs
This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa). I expressly request that the designated record custodian of all covered entities under hipaa identified above disclose full and complete. A hipaa authorization form must be obtained from a patient before their protected health. Exclude the following.
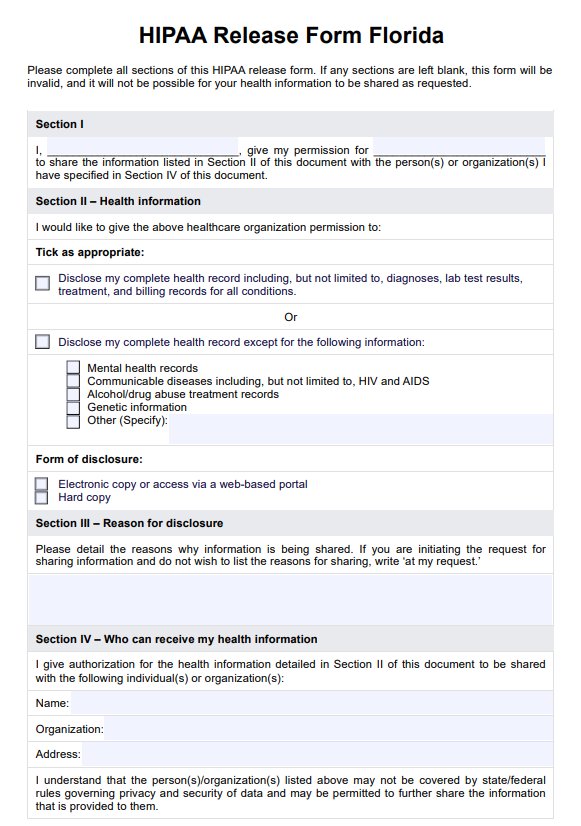
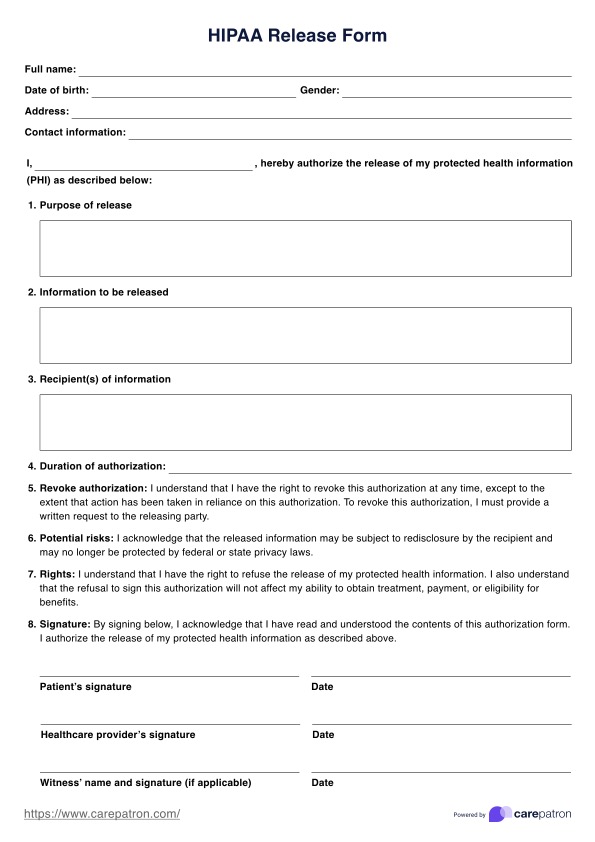
HIPAA Release Form & Example Free PDF Download
Authorize this release to extend to all aspects of testing, diagnosis or treatment. Exclude the following information (initial): A hipaa authorization form must be obtained from a patient before their protected health. Free immediate download of medical relasese form pdf. I expressly request that the designated record custodian of all covered entities under hipaa identified above disclose full and complete.

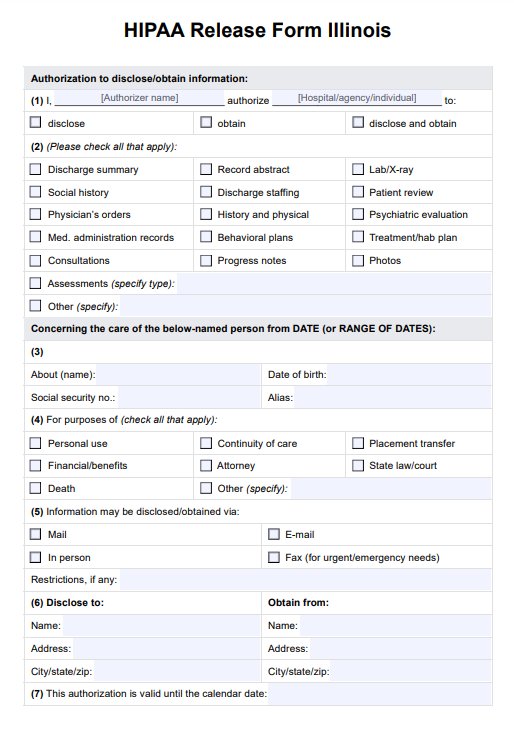
HIPAA Release Template
Authorize this release to extend to all aspects of testing, diagnosis or treatment. Exclude the following information (initial): I expressly request that the designated record custodian of all covered entities under hipaa identified above disclose full and complete. This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996.
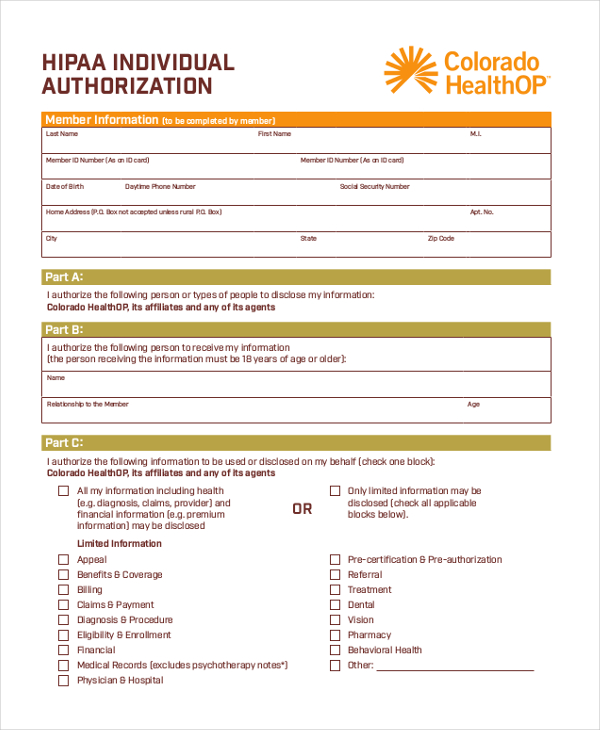
FREE 9+ Sample HIPAA Authorization Forms in PDF MS Word
Free immediate download of medical relasese form pdf. Exclude the following information (initial): This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa). A hipaa authorization form must be obtained from a patient before their protected health. I expressly request that the designated record custodian of all.

Printable Hipaa Form Printable Forms Free Online
A hipaa authorization form must be obtained from a patient before their protected health. Free immediate download of medical relasese form pdf. I expressly request that the designated record custodian of all covered entities under hipaa identified above disclose full and complete. Authorize this release to extend to all aspects of testing, diagnosis or treatment. This form is for use.
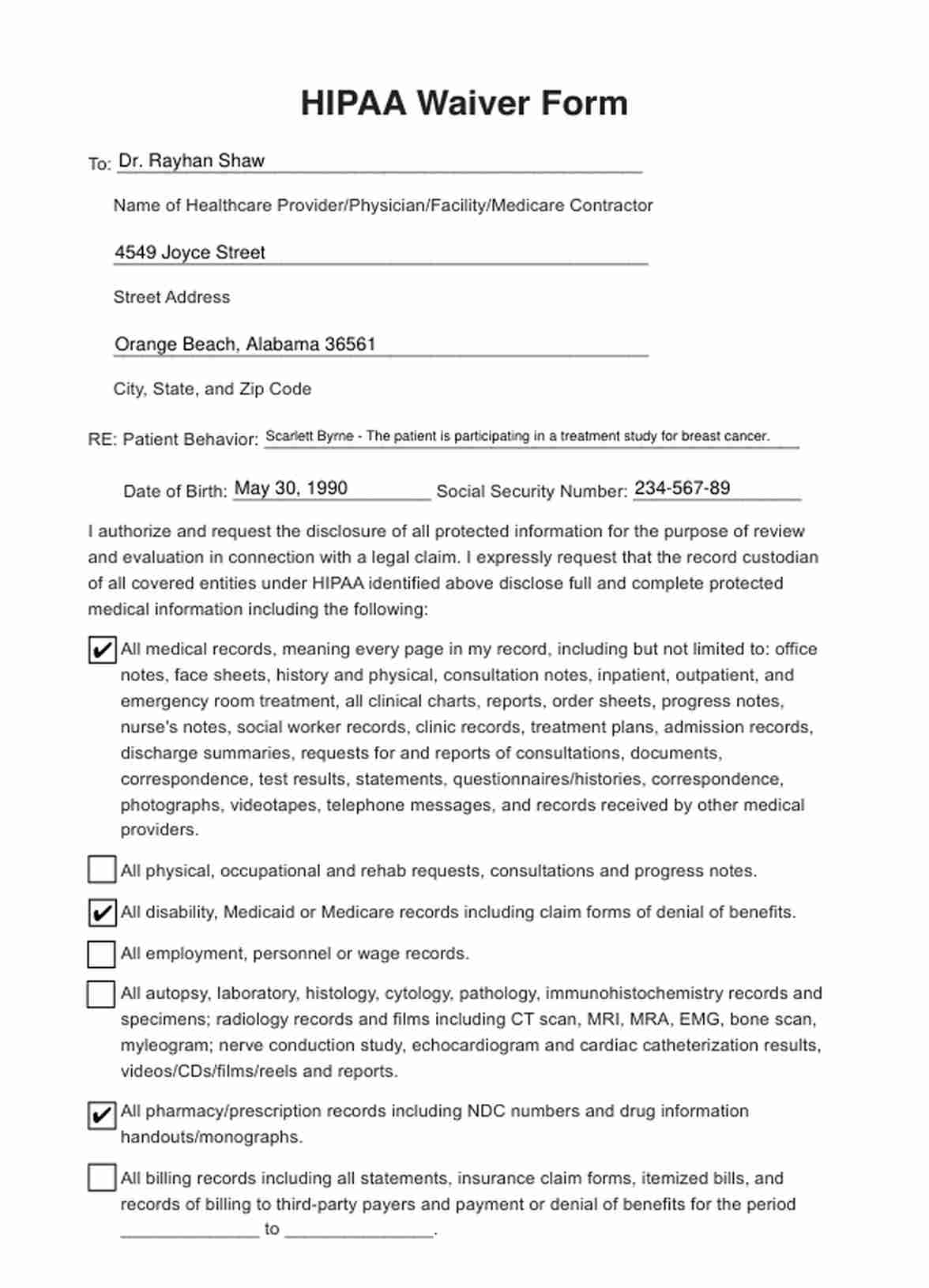
HIPAA Waiver Form & Example Free PDF Download
This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa). A hipaa authorization form must be obtained from a patient before their protected health. I expressly request that the designated record custodian of all covered entities under hipaa identified above disclose full and complete. Exclude the following.
HIPAA Waiver Form & Example Free PDF Download
This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa). Free immediate download of medical relasese form pdf. Exclude the following information (initial): I expressly request that the designated record custodian of all covered entities under hipaa identified above disclose full and complete. Authorize this release to.
Pdf Printable Hipaa Form Printable Form 2024
Free immediate download of medical relasese form pdf. This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa). Authorize this release to extend to all aspects of testing, diagnosis or treatment. A hipaa authorization form must be obtained from a patient before their protected health. I expressly.
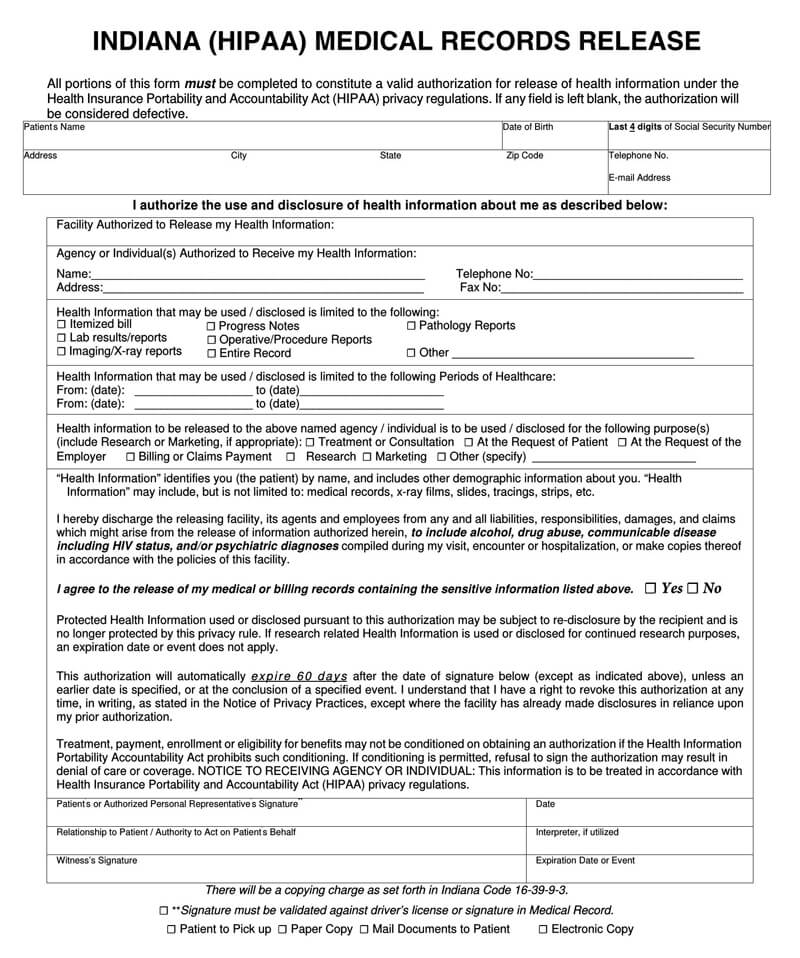
Medical Records Release Hipaa Form Pdf Word Templates Fillable Hipaa
Exclude the following information (initial): This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa). A hipaa authorization form must be obtained from a patient before their protected health. Free immediate download of medical relasese form pdf. Authorize this release to extend to all aspects of testing,.
A Hipaa Authorization Form Must Be Obtained From A Patient Before Their Protected Health.
I expressly request that the designated record custodian of all covered entities under hipaa identified above disclose full and complete. Authorize this release to extend to all aspects of testing, diagnosis or treatment. Free immediate download of medical relasese form pdf. This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa).